



With input from NBC News, the Washington Post, the Hill, Reuters.
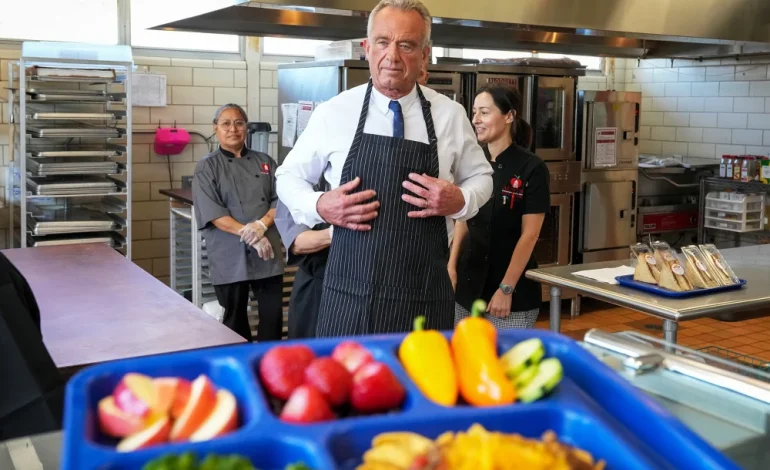
Robert F. Kennedy Jr. just put nutrition back in the spotlight — and he didn’t do it quietly. The health secretary has spent months prodding medical schools to teach more about food, diet and the messy links between what we eat and long-term illness. He threatened to yank funding from holdouts, dangled public praise for cooperators, and now, about 52 schools have signed up to try a new plan that starts this fall.
What the push asks for is pretty simple: medical schools should (1) audit how much nutrition training they already give, (2) name a faculty lead to own nutrition education, and (3) publish a public page explaining how they’ll reach roughly 40 hours of nutrition teaching (or something equivalent). Officials say the effort is voluntary and not a one-size-fits-all curriculum. Think of it as a how-to guide, not a federal lesson plan.
Why 40 hours? For decades, doctors and educators have griped that nutrition gets short shrift. A 2015 survey found med students get about 19 hours of nutrition across four years on average. The problem isn’t new — the American Medical Association flagged it back in the 1960s. So the target is meant to be a big leap forward, not a tweak.
There’s practical logic here. Nutrition plays a role in diabetes, heart disease and other chronic conditions that dominate clinic schedules. Teaching students to spot nutrition problems and to know when to send patients to experts could, in theory, reduce pill scripts and focus more on prevention.
Still, this isn’t a unanimous cheer.
Marion Nestle, a longtime food-and-health scholar, says more training would be “lovely,” but points out the limits. Doctors have short visits with patients. What really matters, she says, is whether clinicians can spot a nutrition issue and then refer patients to a dietitian. That’s where real help happens. Marion Nestle
And then there’s the credibility question. Dr. Adam Gaffney, a critical-care physician and assistant professor at Harvard Medical School, supports adding rigorous nutrition science — but he’s wary of the secretary’s track record. Gaffney says the administration leans toward some “pseudoscientific” ideas, and he worries that would bleed into curricula. He also stresses the social side: people often can’t eat better because of cost or time, not ignorance. Adam Gaffney
The administration reportedly sent schools a letter listing a wide swath of possible topics — 71 of them, according to reporting — everything from dietary supplements to wearable devices to composting and even crop rotation. That list raises eyebrows: some items are clearly core clinical knowledge; others look more like lifestyle or policy electives. Officials say they offered suggestions, not mandates.
Which schools? A handful already named publicly include the likes of George Washington University, Tufts and the University of Oklahoma College of Medicine, among others. They’ve agreed to assess, appoint leads and post plans for the 40-hour goal. George Washington University Tufts University University of Oklahoma College of Medicine
Two big associations — the American Medical Association and the Association of American Medical Colleges — are expected to weigh in. The administration says it’s coordinating with them, and they’ll likely help shape how any new nutrition content fits into existing medical training. American Medical Association Association of American Medical Colleges
Critics also flag the political vibe. Some schools reportedly balked because they didn’t want to be seen as signing onto a partisan program. Kennedy and the Education Secretary framed this as part of a larger “Make America Healthy Again” push — a brand that can make university leaders twitchy about academic freedom.
Let’s be blunt about the trade-offs. Packing 40 hours of new content into an already full curriculum is awkward. Medical students juggle anatomy, pharmacology, clinical rotations, licensing exam prep — and those rotations are where clinicians learn to manage real patients under time pressure. So adding nutrition means either trimming something else or shoehorning new material into packed schedules.
There’s another structural point: physicians aren’t nutrition specialists. The smarter route may be clearer screening tools and better referral pathways to registered dietitians and community nutrition programs. Nestle’s point echoes here: doctors need to know when to act and whom to call.
Will this change what patients see in the clinic? Maybe. If med schools actually deliver rigorous, evidence-based nutrition training and pair it with better primary-care staffing and insurance coverage for dietitians, patients could benefit. But if the push morphs into a patchwork of trendy diets, unvetted supplements and political theater, the net gain will be small.
The idea that doctors could be better trained in nutrition is not controversial. The tricky parts are who decides what “better” means, how schools squeeze it into curricula, and whether the end result leans on solid science or slides into politics. This initiative will be judged not on bold targets or press conferences, but on whether it leaves future physicians better able to help patients eat — and whether patients actually get the support they need to do it.



The latest news in your social feeds
Subscribe to our social media platforms to stay tuned